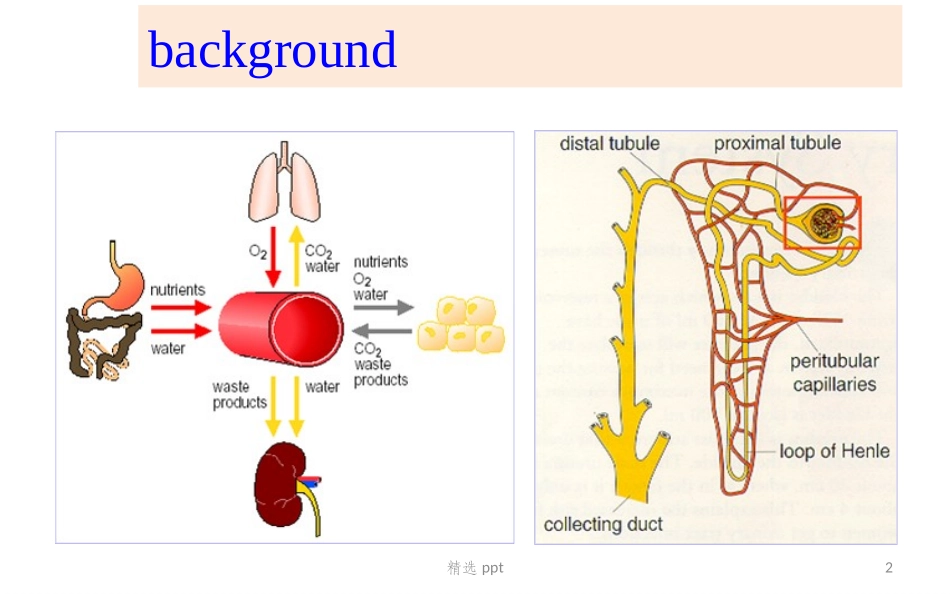
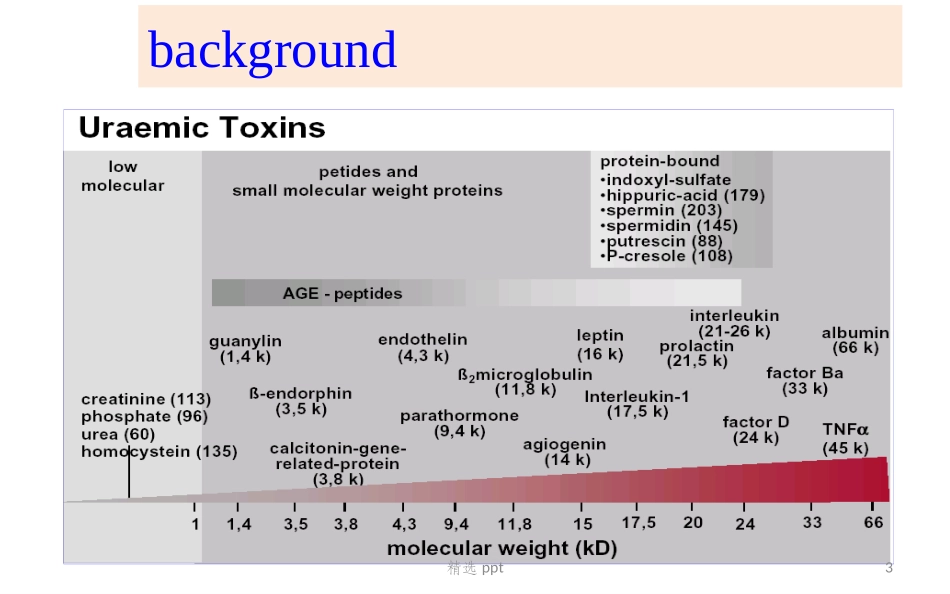
重症血液净化:Q&ACriticalContinuousBloodPurification重症医学科1精选pptbackground2精选pptbackground3精选ppt1970’s……1980’s…2000’sIntermittentHemodialysisContinuousRenalReplacementTherapyNephrologistIntensivist肾脏替代肾脏支持非肾脏疾病background4精选pptcontentDosingTimingModality5精选ppt1Modality:原理0408012010102103104105ureacreatinineVit.B12ß2-MalbumineClearance(ml/min)MW(dalton)diffusionconvectionadsorptionKidneyIL-1TNFIL-6IL-8小分子(MW<500)中分子(MW500~5000)大分子(MW>5000)Ledebo,ARRT19996精选ppt1Modality:Ultrafiltration7精选ppt1Modality:SCUFRemovalofwaterisdonebyUFNoSubstitutionliquidisusedUsedmainlyforCHF+FluidOverloadQf=5~15ml/hQb=100~250ml/h8精选ppt1Modality:Diffusion9精选pptCVVHDTheprinciple(clearances)isDiffusionEliminatemainlySmallMoleculesNetFluidRemovalisdesiredUsedofSterileDialysateSolution1Modality:CVVHDQd=15~60ml/hQb=100~250ml/h10精选ppt1Modality:Convection11精选pptTheprinciple(clearances)isConvectionEliminateSmall,Mid+LargemoleculesNetFluidremovalifdesiredInpre&/orpost-DilutionFluidsarereturningbefore&/oraftertheFilterinsidethevenousline1Modality:CVVHF~HVHFQf=15~60ml/hQb=100~250ml/h12精选pptTheprinciple(clearances)isConvection+DiffusionEliminateSmall+MidmoleculesNetFluidremovalifdesiredUseofSterileDialysate+ReplacementSolutionsCVVHDF1Modality:CVVHDFQf=10~30ml/hQd=15~30ml/hQb=50~200ml/h13精选ppt1Modality:CRRT模式的转换SCUFCAVHCVVHCAVHDCVVHDCAVHDFCVVHDF+置换液+血泵+血泵+血泵-置换液+透析液-置换液+透析液+置换液+置换液超滤率↑溶质清除↑超滤率↑14精选ppt1Modality:吸附/置换15精选ppt1Modality:TPE/HP陈香美.血液净化标准操作规程[M].第1版,北京:人民军医出版社,2010.类别主要诊断PEHP风湿SLE(脑)、难治性类风湿关节炎、系统性硬化症、抗磷脂抗体综合征●神经MGs、Guillain-Barrèsyndrome、Lambert-Eaton肌无力综合征、多发性硬化病、慢性炎症性脱髓鞘性多发性神经病等。●消化重症肝炎、严重ALF、肝性脑病、胆汁淤积性肝病、高胆红素血症●√血液多发性骨髓瘤、高γ-球蛋白血症、冷球蛋白血症、巨球蛋白血症、TTP/HUS、新生儿溶血、白血病、淋巴瘤、重度血型不合的妊娠、自身免疫性血友病A等。●肾脏抗肾小球基底膜病、急进性肾小球肾炎、难治性局灶节段性肾小球硬化症、系统性小血管炎、重症狼疮性肾炎等●CKF中毒药物过量(如洋地黄中毒等)、与蛋白结合率高的毒物中毒●√代谢纯合子或半纯合子型家族性高胆固醇血症等●皮肤大疱性皮肤病、天疱疮、中毒性表皮坏死松解症、坏疽性脓皮病●银屑其他MOF、自身免疫性甲状腺疾病、(器官移植)●√16精选ppt1Modality:CRRT/HP曹钰,柴艳芬,陈玉国,等.血液净化急诊临床应用专家共识[J].中华急诊医学杂志,2017,26(1):24-3617精选ppt1Modality:CRRT/HP蛋白结合率:游离CRRT,结合HP低高分布容积Vd小(血管内)CVVHDFHP/PE大(血管外)HP+CVVHTPE+CVVH强调早期CBP模式特点HP游离的毒物CRRT,结合的毒物HPTPE清除体内已与血浆蛋白结合的毒素,补充白蛋白、免疫球蛋白、凝血因子等CVVH血流动力学稳定、有效清除中小分子物质和消除组织水肿、置换液补充个体化,利于营养支持,更适于中毒所致MODS曹钰,柴艳芬,陈玉国,等.血液净化急诊临床应用专家共识[J].中华急诊医学杂志,2017,26(1):24-3618精选ppt1Modality:Spesis/MODS体外血液净化能改变SIRS吗?在Sepsis-AKI患者中,是否应该使用比常规剂量(20~25ml/kg.h)更高的超滤剂量?在Sepsis/MOF发生AKI时,CRRT治疗是否优于IRRT?AKI+脑水肿(CVVH)AKI+高代谢状态(CHFD)AKI+充血性心力衰竭(SCUF)超滤是否可作为肾脏之外MOST手段?心脏(FO及利尿剂抵抗的ADHF:CVVH;血流动力学不稳定:SLED)ARDS(CVVH)肝衰竭(HP/TPE/CFPA/MAR...